
This is Part 1 of the unique PSC exclusive Doctor-Patient Deep Dive programming series with collaborative discussions between patients and surgeons.
Dr. Mindy Haws moderates a lively and informative discussion. Breast Implant Illness (BII) and Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) have gotten a lot of press lately. Women across the country with breast implants are suffering from a myriad of symptoms with no readily apparent cause. While more is known about the latter and, more importantly, there is a way to test for it, breast implant illness is more or less a diagnosis of exemption.

It is frustrating for both the patient and the surgeon. The bigger question, however, is why do only some women experience breast implant illness? And is there a way to bridge the gap between a patient’s understandable fear, anxiety and anger, and the surgeon’s ability to safely deliver on their desires? Dr. Melinda Haws of Nashville, TN heads up the task force for breast implant illness for the American Society For Aesthetic Plastic Surgery (The Aesthetic Society). She leads a deep dive discussion panel of women on the best ways to maximize breast implant patient safety.
What is Breast Implant Illness?
Dr. Pat McGuire is a board certified plastic surgeon in St. Louis, MO. She is on The Aesthetic Society task force on BII. Her experience with breast implant illness is that patients are coming into her office suffering from a multitude of symptoms for which there is no direct cause. The most common complaints that she hears are:
- fatigue
- joint pain
- GI problems
- anxiety
- restlessness
- changes in their hair
- body odor
By the time that these women get to her, they have typically had extensive workups for which they may have spent thousands of dollars out of their own pockets. And yet, none of these tests have revealed an underlying cause for their symptoms. They are usually at “the end of their rope.”

Breast Implant Illness is the term used to describe this group of women with this collection of symptoms that they attribute to their breast implants. “We don’t know a lot about it. There’s not a blood test that can be done for it or x-rays that can be taken to diagnose it,” explains Dr. McGuire. These women have real symptoms and find themselves having a hard time getting people to take them seriously.
Breast Implant Illness: A Patient’s Perspective
Jamee Cook directs a breast implant victim advocacy and patient support group on Facebook and started a FB support site for BIA-ALCL as well. Her story is all too familiar. She was an active mother of two who was working as a paramedic when she got her PIP saline breast implants in 1998. By year 3, however, she began to suffer from fatigue, lymphadenopathy and recurrent fevers. It “never once crossed my mind that I needed to go see my plastic surgeon,” says Ms. Cook. It never occurred to her that her symptoms could be caused by her implants. The doctors that she consulted simply chalked up her symptoms to the rigors of her job and of being a working mother.
But things got worse. She was eventually diagnosed with auto-immune Hashimoto’s disease and thought this was the answer. Even so, the thyroid medicine did not relieve her symptoms. She ultimately quit her job after having her third child. In 2012, one of her implants ruptured, but she didn’t have the money to fix it for 3 years. This wound up being a god send. When she went in to meet her surgeon, he said that he would replace her implant. She wasn’t sure that she wanted to take this route, but the conversation did spur her to go in search of her implant card to find out what type of implants she had.
This is when she discovered that she had the PIP saline implants which were low quality devices. By this point, she had developed a host of other symptoms including chronic sinus infections, anxiety, anger issues that affected her relationship with her kids and husband, arm/hand numbness, and migraines. As she began to do research and saw the generalized lists online from other breast implant illness sufferers, she became convinced that her implants were the problem. She decided to have both the implants and the capsule removed. “I would say that 80-90% of my symptoms went away immediately,” explains Ms. Cook. The brain fog that had made it impossible for her to process the medical journals that she loved lifted. Her relationship with her husband and kids improved. She got off all of her medications except her thyroid medication. When she had her implants she was a “different person. Without them, she went back to normal.
Seeing Your Surgeon for Suspected Breast Implant Illness
Ms. Cook did not want to go back to her implanting surgeon once she found out that “he had put devices in me that had not been approved by the FDA.” This is understandable, but Dr. McGuire finds that patients typically come to her because their original surgeon won’t remove the implants since they “look great.” This has been a huge problem for breast implant illness sufferers.
For the surgeon, the issue can be that patients don’t want to disappoint him or her. Dr. Haws believes that her patients are reluctant to come to her and say: “I know that you did these in good faith but I really don’t want these implants.” She typically sees other people’s patients for implant removal.

Furthermore, it has been difficult to track the patients with breast implant illness who’ve had their implants removed. The “I used to have breast implants, but now the implants are gone” patients are like happy patients – the surgeon doesn’t hear from them again. “Once you’re happy, patients go on about their lives so it’s hard to track,” says Haws. “This is why it’s important to talk to each other and see how your life improved.”
Bridging the Communication Gap
One of the goals of the task force, explains Dr. Haws, is to bridge this communication gap between breast implant illness patients and plastic surgeons. “It’s interesting because cars are safe, but people die in car crashes everyday,” says Dr. Haws. The hard thing for plastic surgeons is that there have been so many studies done on implants. A breast implant is technically the most studied medical device in the world. Plastic surgeons know that the device is safe. And yet, breast implant illness and BIA-ALCL are real. “We have to continue to on go with the research.”
Dr. Jennifer Kessmann of Dallas, TX is a Board Certified Family Medicine physician who is also functional medicine certified. For her, it is important to remember “medical evidence is always evolving.” Dr. Haws agrees and points out that in addition to the difficulty in tracking breast implant illness patients post implant removal, there have been no great studies done on breast implant illness. The Aesthetic Society is trying to change this.
Who Develops Breast Implant Illness & Why?
“Implants are not poisonous,” explains Dr. McGuire. There are 300,000 women every year who get a breast augmentation, and there are at least 50 million women globally with breast implants. If all of them developed symptoms or if even 10% did, “we’d have been paying attention a lot sooner.” But many of these patients do feel better once the implants are removed, so even though it’s a small percentage of overall breast implant patients does not mean that it’s not a real percentage. The important question: How do we figure out who will develop breast implant illness and who will not?
It’s vital for plastic surgeons to recognize the symptoms and not dismiss them. In the past, surgeons tended to go one of two ways:
- take the patient right into surgery and put her through an expensive removal process
- dismiss the patient with a “You are OK, nothing is wrong.”
While it’s true that not every woman who gets a headache has breast implant illness, this is a real disease. So, plastic surgeons need to really listen to their patients, and evaluate the big picture.
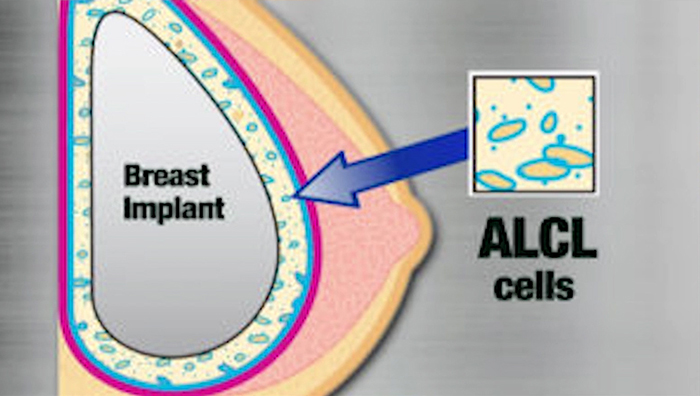
BIA-ALCL: A Patient’s Perspective
Breast Implant-Associated ALCL is a slightly different scenario than breast implant illness. Raylene Hollrah is a 12 year breast cancer survivor who developed BIA-ALCL after her 5th year check up. Her journey was totally different than Ms. Cook’s.
She was diagnosed with breast cancer at the age of 33 and had a bi-lateral mastectomy, choosing not to do immediate reconstruction. She waited a year and half and did her research. She saw 3 plastic surgeons and finally settled on the one with whom she felt most comfortable. She chose a textured implant that was approved by the FDA and agreed to be part of a ten year study that was being conducted. She felt as if she was extremely educated coming into the process.
For the first 5 years, she was not symptomatic. “I was very happy,” explains Ms. Hollrah. It wasn’t until the end of that 5th year that she developed swelling. She was diagnosed with BIA-ALCL and was shocked to realize that her implants had given her cancer because she never felt sick. The National Center for Health Research in 2018 followed 300 women, 89% of which improved after their implants were removed. It’s a small study, but once Ms. Hollrah had her implants removed, the cancer was gone.
BIA-ALCL is Sneaky, but Definitely Treatable
The problem with BIA-ALCL is that it does not necessarily make the patient feel bad at first. This is what makes it so sneaky. If BIA-ALCL is caught early, as in Ms. Hollrah’s case, it is readily curable. This is the good news. The other good news is that there is something definitive that can be done to diagnose BIA-ALCL. The surgeon draws fluid, sends in a piece of the breast capsule to pathology, and gets back a clear diagnosis. “That’s the piece that we’ve tripped over with breast implant illness,” explains Dr. Haws. Patients feel terrible, but she doesn’t have a lab test that she can order. Breast implant illness is more of a diagnosis of exclusion.
En Bloc Capsulectomy
One of the more difficult aspects of breast implant illness for surgeons and patients is the concept of “en bloc” capsulectomy. Patients come in convinced that their implants are making them sick, requesting the implants to be removed, as well as the capsule taken out ” en bloc.” This concept has been propagated by some surgeons, and social media with no real science to support. In fact, enbloc capsulectomy can sometimes result in increased patient morbidity and complications including removal of normal wall muscle and lung punctures with no real known added benefit; there is a distinct dichotomy between “enbloc” vs. expert breast surgeons preferred technique called “Precise capsulectomy” were the capsule is precisely removed under direct vision taking care to remove the capsule but not injure other tissues. Typically the implant is removed at some point during the capsulectomy. Patient exploitation by some surgeons has been present with these “enbloc” recommendations often inferring only a few surgeons have the training and skill, and this justifies extremely high surgical fees etc.
En Bloc Can be Dangerous
The reason that enbloc removal is sometimes dangerous, explains Dr. McGuire, is because the posterior part of the implant may be very close to the lungs. If the patient has an implant above the muscle with a thicker capsule, it is easy for her to remove the whole capsule. She will gladly take it out, and give the patients photos of the capsule and the implants.
However, if a patient has an implant below the muscle, it can be more difficult because the space between the ribs and the lung is not that deep. If she tries to take the capsule out, it’s akin to removing wall paper from dry wall. In the posterior section by the ribs, that dry wall may be too close to the lung so that removing it could collapse that patient’s lung or take off a lining of the ribs. If the patient has BIA-ALCL, the risk is worth it. Otherwise, it’s not always worth the risk.
“I treat every patient how I would want to be treated,” explains Dr. McGuire. Patient safety is paramount, but when she tries to explain this to breast implant illness sufferers, oftentimes “they don’t listen.”
Another issue discussed in this Deep Dive is that plastic surgeons can not always guarantee that they can safely remove the capsule enbloc, yet the minute that they try to explain this to the patient, the “curtain comes down.” How is it possible for surgeons to keep the conversation open and communicate that they just want to help?
Ms. Cook recognizes that surgeons are in a hard position; however, so are patients who often still think that doctors know best and who are reluctant to open a confrontational conversation, but she also knows that “no one can guarantee an en-block removal,” because if the thin capsule tears, it’s no longer en bloc. Nevertheless, in this situation he or she can still remove the whole capsule. Since 40-50% of BII patients are have saline implants. A frequent question is in a completely thin, normal appearing capsule is there anything pathologic there to cause illness. All implanted human implants including breast implants will have bacteria detected via DNA analysis in the normal situation. The question is when normal becomes abnormal. It is not know fully, but breast implant and capsular contracture experts/ scientists believe the a thin normal appearing capsule do not carry bacterial loads that could be high enough to cause disease. This is currently being studied and more data will be available in the future.
Sometimes patients don’t realize that there are no guarantees. They simply think that a surgeon who can not promise en bloc is a terrible surgeon. Patients need to be educated, “because they may potentially be missing out on a surgeon who’s highly skilled,” explains Ms. Cook. Dr. Kessman believes that as long as the surgeon is coming from a place of “I want to help and will take the capsule out if I can,” this is a different story than “it doesn’t matter if the capsule is removed or not.” If the surgeon explains that he or she will do 100% of what can be done safely then this goes a long way towards bridging this communication gap.
The Answer Lies in Patient Education
A takeaway point for both surgeons and patients is that this “should not be a quick conversation with your plastic surgeon,” shares Haws. “There should be some back and forth and why your case is different from the other cases they see and what can’t be done and what can be done.” Furthermore, anyone who guarantees anything is simply blowing smoke. There is really no way for the patient to know if the surgeon did what he or she says except trust. “It’s gotta be a partnership.”
Both the advocates and surgeons agree that it is vital to see a board certified plastic surgeon, and to get more than one opinion. Patients also need to do their homework and know what type of breast implant that they have.
How Surgeons Work Has Changed in the Last 5 Years
The proliferation of information on breast implant illness and BIA-ALCL has changed how plastic surgeons work today. Thanks to YouTube, patients have a higher tolerance for gory surgical photos. Dr. Haws makes it a point to take inter-operative photos. It’s good for her business as it relieves patient anxiety and the photos also become part of the medical record. Dr. McGuire sends every capsule that she removes to the pathologist. This was not routine for her until about 5 years ago.
Both Dr. Haws and Dr. McGuire encourage their patients to come in if anything feels weird or off. They both want there to be an on going conversation. Since BIA-ALCL, every patient who comes in for a follow-up is given an update on the disease so that they know the early signs. If the patient has textured implants, Dr. Haws sees that patient yearly. Dr. McGuire offers free yearly follow-ups, and sends her patients a reminder to let them know about BIA-ALCL. They both also have recently purchases a high resolution ultrasound, helping greatly with the screenings as it allows the surgeon to detect any fluid around the shell.
The goal of all of these changes is to reduce patient anxiety. It is critical for patients to remember that a great plastic surgeon is always on her side.










Facebook
Twitter
Instagram
YouTube
RSS